Healthcare AI Industry Report
Practical guidance for industry leaders as healthcare AI moves toward deployment at scale.

The 2026 Healthcare AI Industry Report translates the rapidly expanding evidence base into practical guidance for industry leaders as healthcare AI moves toward deployment at scale.
Ethan Goh, Adam Rodman, Jonathan H Chen
Supported by






Questions Industry Leaders are Asking
This report addresses and draws on on 3 questions shaping Healthcare AI deployment in 2026.
Is this technology safe for patient care?The field cannot yet answer definitively. Failures that significantly impact clinical care, including hallucination, omission, automation bias, and silent degradation, are not well represented in current benchmarks.
How do we improve human–AI collaboration?Physicians using AI are not yet reliably outperforming AI on its own, and in several studies, they underperform it, raising urgent questions about human-AI workflow design. Integrating AI into clinical workflows to improve decisions, reduce errors, and support clinicians at scale requires better collaborative interfaces and prospective evaluation that measures patient outcomes.
What system-level conditions can ensure healthcare AI creates real-world value?Model capability is only one part of the answer. The next priority is building the institutional infrastructure around AI.
Key Takeaways
What healthcare AI leaders should know in 2026
Chapter 1
Capability is advancing faster than safety evaluation
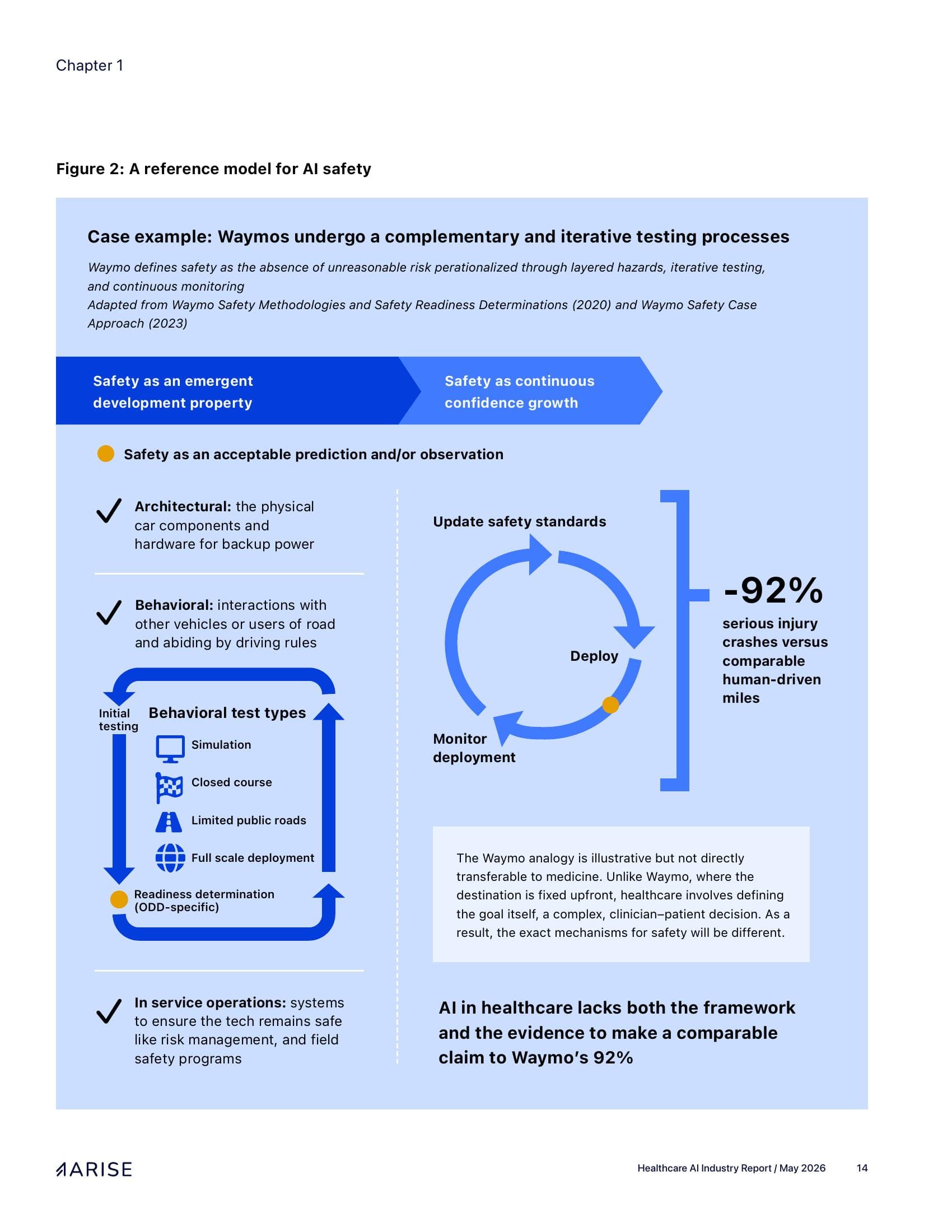
Capability is outpacing the benchmarks that evaluate it.
Healthcare AI is advancing faster than the benchmarks used to evaluate it. As models saturate existing benchmarks and cross performance thresholds across more tasks, the urgent need is to understand how these systems fail in healthcare, especially for generative and agentic AI.
Safety must be explicitly evaluated.
Early results from ARISE's Medical AI Superintelligence Test (MAST) show that even the most capable models frequently produce harmful recommendations, and that systems performing well on knowledge and workflow tasks can still fail in ways that matter for patient care.
Organizations need to invest in internal evaluation capacity.
Institutional maturity is increasingly defined by whether a system has the right data pipelines and evaluation expertise in place.
Chapter 2
Deployment is happening. Outcomes are next.
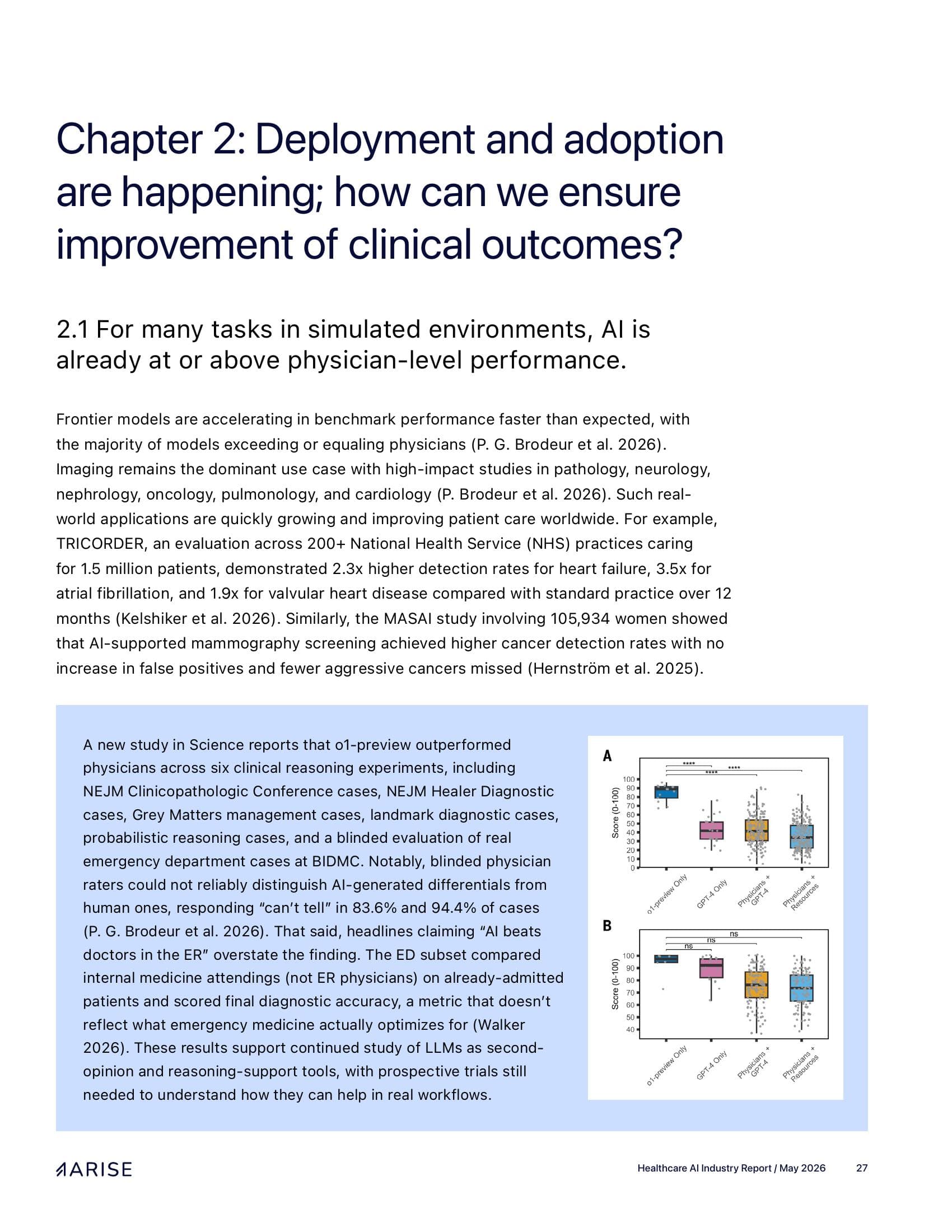
Physicians using AI are not yet reliably outperforming AI alone, and in some studies, underperform it.
Optimizing human-AI collaboration requires deliberate tool and workflow design, paired with real-world studies that show where models and clinicians each fall short.
Human-in-the-loop can be flawed at scale.
Human oversight will remain essential, but where access, clinician time, or resources are constrained, requiring human review for every AI-supported task creates the appearance of safety while limiting impact.
The next stage of evidence will be prospective.
Google's Articulate Medical Intelligence Explorer (AMIE) studies illustrate a progression from simulated consultations to a prospective real-world feasibility study at BIDMC, and now to a nationwide randomized study with Included Health to evaluate conversational AI in real-world virtual care workflows.
Chapter 3
System-level conditions can stand between capability and value
Without federal guardrails, liability moves downstream.
The current US policy environment orients toward faster AI deployment and reduced regulatory friction. Without clear federal guardrails, liability can move downstream to the clinicians, health systems, and vendors closest to deployment.
Privacy and governance have not kept pace.
Privacy and governance frameworks have not kept pace with frontier healthcare AI systems. Health systems need named institutional ownership for AI governance, clear approval pathways, and sanctioned tools that reduce the incentive for clinicians and staff to use informal AI tools.
Payment incentives will shape healthcare AI as much as model capability.
In the near term, AI will scale most easily where the business case fits existing reimbursement models. These applications produce real operational value, but also risk using AI to optimize legacy workflows rather than redesign care around measurable improvements in outcomes and access.
Recommendations by stakeholder
What health systems, builders, investors, and researchers can do now
Health systems
- Designate a single institutional owner for AI evaluation.
- Before deployment, specify the intended workflow: who sees the AI output, when it appears, how uncertainty is displayed, what clinicians are expected to do with disagreements, and when escalation is required.
- Close the shadow AI gap and ensure BAAs cover agentic and chained workflows before deployment.
Builders
- Report failure modes alongside performance and build evaluation into the product so customers can monitor performance against their own data.
- Design interfaces with clinicians from the start.
- Design for privacy beyond de-identification and prioritize deep workflow integration.
Investors
- Make evaluation infrastructure part of due diligence — either build an in-house toolkit or partner with trusted evaluators.
- Treat workflow evidence as part of product maturity.
- Stress test thesis against payment-model risk and EHR-bundling risk.
Researchers
- Prioritize benchmarks that capture harm severity, omission, and calibration under uncertainty over aggregate accuracy.
- Compare alternative collaboration designs for the same task, rather than treating “AI plus clinician” as a single intervention.
- Develop accountability frameworks that delineate liability across developers, institutions, and clinicians when AI-assisted decisions cause harm.
How to cite
Perez, A., Tusty, M., Morgan, D., Liu, C., Wegner, L., Dutta Gupta, N., Kanjee, Z., Jain, P., Mehta, R., Walton, C., McCoy, L., Nateghi Haredasht, F., Eltahir, A. A., Bielick, C., Griot, M., Lopez, I., Lacar, K., Schoeffler, A., Shah, P., Fathy, R., Han, B., Zheng, A., Anyaegbuna, C., Wu, D., Ravi, V., Brodeur, P., Handler, R., Manrai, A., Zwaan, L., Rodman, A., Goh, E., & Chen, J. (2026). The 2026 Healthcare AI Industry Report. ARISE, Stanford, CA.
Acknowledgements
The authors would also like to thank Abigail Foresman, David J. Wu, John Emmett Worth, Macy Toppan, Marshall Berton, Samuel O'Brien, Katherine Ropers, Sarah Jabbour, and Zina Jawadi for their contributions. They would especially like to thank Michi Turner, Rebekah Lee, and Joel Koh for the report design.